| Home News and Events |
|

eNeuroMaximizing minimally invasive brain tumor surgery
Pankaj Gore, M.D.
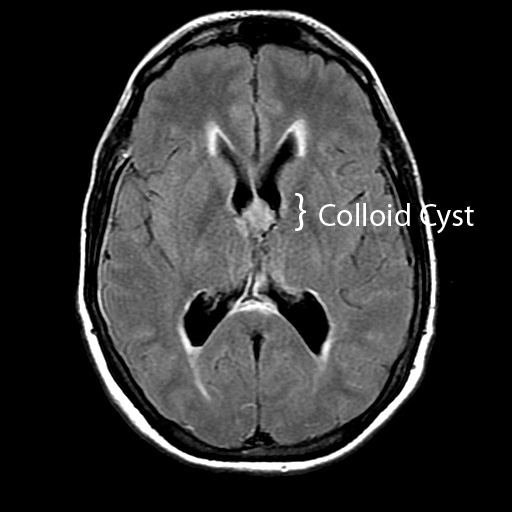
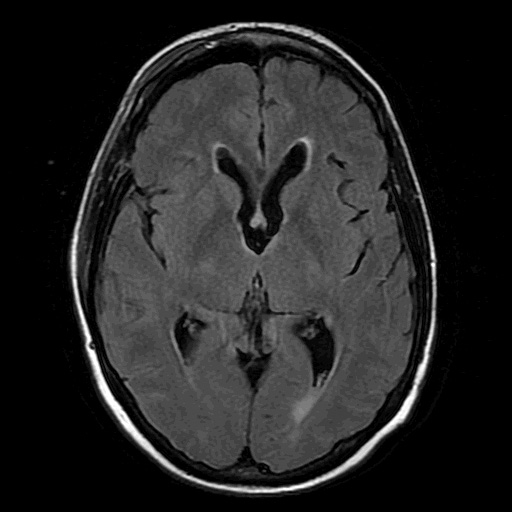
Co-medical director, Providence Cranial Services Case 1: A 48-year-old woman was found in a comatose state in her car. She had no history of headaches, nausea or vomiting. Her Glasgow Coma Score was 7 of 15. A CT scan taken at Providence St. Vincent Medical Center revealed a massive ventriculomegaly and a 1.4 cm colloid cyst in the anterior third ventricle (Figure 1), which was causing obstruction of bilateral foramina of Monro. Bilateral extra ventricular drainage catheters were emergently placed to divert cerebrospinal fluid. Over three days the patient demonstrated marked neurological recovery with a return to baseline. On the fourth day she underwent an uncomplicated resection of the colloid cyst via a right frontal endoscopic approach (Figure 2). She was discharged within 48 hours of surgery, having made a full neurological recovery.
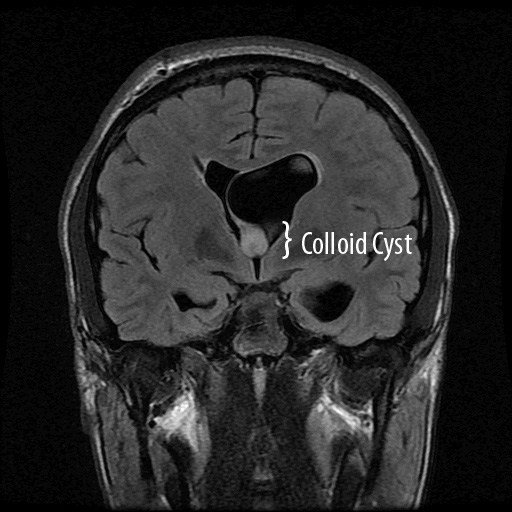
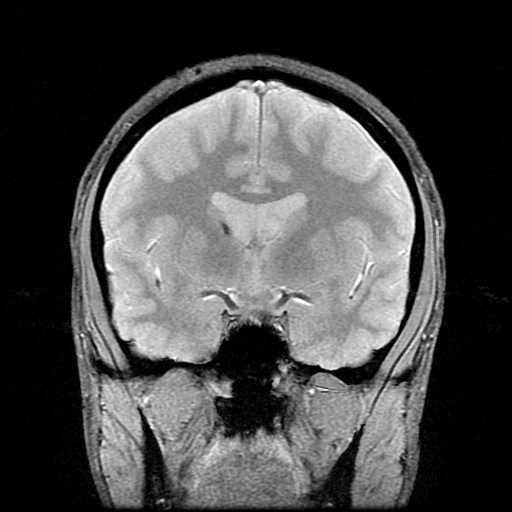
Case 2: A 17-year-old competitive cyclist presented to an outside hospital with a four-day history of progressive headaches, nausea, vomiting and lethargy. Imaging demonstrated marked hydrocephalus and a 1.2 cm colloid cyst in the anterior third ventricle obstructing bilateral foramina of Monro (Figure 3). The hospital’s neurosurgeon placed a unilateral extra ventricular drain, and the patient was transferred to Providence St. Vincent Medical Center neurosurgery for further care. He underwent an uncomplicated endoscopic colloid cyst resection and was discharged home three days later (Figure 4). Today he is neurologically normal and has returned to competitive cycling. Colloid cysts are epithelium-lined lesions that arise in the anterior third ventricle. Though technically non-neoplastic, they account for 1 percent of brain tumors and 15 to 20 percent of intraventricular lesions. The cyst’s consistency can vary from gelatinous to chalk-like. These lesions are benign and slow-growing, but in rare instances are known to cause sudden death due to acute obstruction of cerebrospinal fluid flow at the foramina of Monro. The most frequent presentation is headache, but memory difficulty, visual disturbance, cognitive disturbance, gait difficulty and urinary incontinence have all been reported. A number of colloid cysts are also incidentally found. Indications for treatmentThe two management options for patients with colloid cysts are surgery and serial radiographic imaging with clinical observation. General medical condition permitting, all patients with symptomatic colloid cysts should be treated. Younger patient age, increasing cyst size, increasing ventricular size and increased signal on T2-weighted MRI (indicating softer, gelatinous contents) are all more likely to be associated with a symptomatic colloid cyst.1 Incidentally discovered colloid cysts can present with normal or enlarged ventricle size. Although some authors have recommended observation in asymptomatic patients with enlarged ventricles,2 the primary study supporting this management strategy is weakened by the large number of patients who were lost to long-term follow-up. Videos Endoscopic resection of a colloid cyst  Cyclist Phelan Kostur describes the symptoms of his colloid cyst to KPTV. I recommend surgical treatment of incidentally found colloid cysts if the ventricles are enlarged for the patient’s age, without another underlying cause, or if the cyst is 10 mm or larger. Asymptomatic patients with incidentally found colloid cysts smaller than 10 mm and normal-sized ventricles can be followed with serial neuroimaging. Surgical approachesThe first successful craniotomy to remove a colloid cyst was performed by Dandy in 1921. For many years craniotomy, via either a transcortical frontal approach or an interhemispheric transcallosal approach, remained the mainstay of surgical treatment. The development of intracranial stereotaxis allowed the cyst’s contents to be removed through a minimally invasive needle aspiration. Though effective, this technique is plagued by high rates of cyst recurrence, as the secretory cyst lining is not addressed. The development of endoscopic colloid cyst resection was a major advance in the treatment of this disorder. This technique was somewhat rudimentary when first reported almost 30 years ago. Since then, instrumentation and surgical techniques have evolved, and today endoscopic resection is an elegant first-line approach to treat the vast majority of colloid cysts. Modern endoscopy requires a skin incision measuring only 1.5 cm and a cranial burr hole of 8 to 9 mm diameter to safely and effectively remove a colloid cyst. Several retrospective studies comparing craniotomy with endoscopic colloid cyst resection have shown that the minimally invasive approach results in statistically significantly shorter operative times and hospital stays, fewer postoperative complications, a lower rate of ventriculoperitoneal shunt dependence and faster return to work.3,4,5 Craniotomy versus endoscopic resectionThe major criticism of endoscopic colloid cyst resection has been the increased rate of cyst recurrence. This is generally a problem only when subtotal resection with cauterization of the cyst wall remnant is employed. In experienced hands with the goal of radical cyst wall resection, rates of recurrence for this approach are as low as with craniotomy.6, 3 Conversely, a recent series examining craniotomy with interhemispheric approach for colloid cyst resection showed low complication rates, equivalent to endoscopy, and no recurrences long-term.7 Neurosurgeons continue to debate the superiority of endoscopic colloid cyst resection versus craniotomy. Due to the steep learning curve for endoscopic techniques and the rarity of these lesions, the skills to endoscopically remove these tumors are still not a part of mainstream neurosurgery. Optimal treatment decisions can be made by surgeons proficient in both open and endoscopic techniques. In my experience it is the rare colloid cyst that cannot be resected safely and completely with endoscopy. Normal ventricle size is generally not an obstacle to endoscopic resection. I reserve craniotomy for large lesions (2 cm or larger) with calcified contents, or for lesions located more posteriorly within the third ventricle where safe access through the foramen of Monro is less feasible. The presented cases demonstrate that although colloid cysts are rare benign brain tumors, they can cause acute or subacute life-threatening neurological deterioration. In experienced hands, endoscopic colloid cyst resection is curative, with reduced morbidity, operative time and postoperative hospitalization as compared to open craniotomy. References
Past articles by Pankaj Gore, M.D. |
||||||||||||||||||
|
||||||||||||||||||
|
Copyright © 2026 Providence Health & Services. All rights reserved. Clinical Trials | Quality and Outcomes | News and Events | About Us | Contact Us | Make a Referral |
||||||||||||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}