| Home News and Events |
|

eNeuroAneurysm: When to clip, when to coil
Vivek Deshmukh, M.D., F.A.C.S.
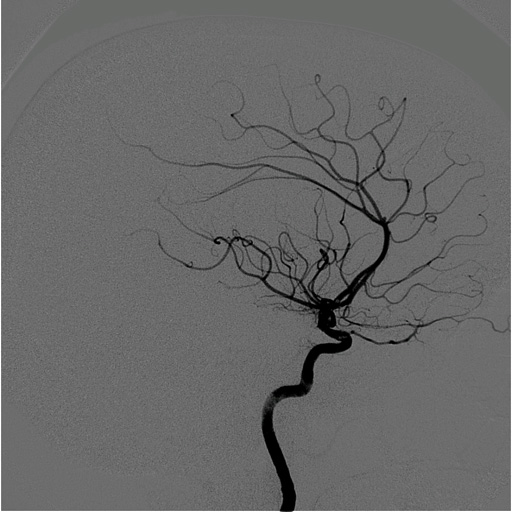
Medical director, Providence Neurointerventional Services Case reportA 73-year-old female presented with a one-week history of right orbital pain, three days of diplopia and a two-day history of right-eyelid ptosis. She notified her primary care physician, and an urgent MRI brain scan was ordered. MRI of the brain and MR angiogram of the head showed a right posterior communicating artery aneurysm compressing on the third cranial nerve (oculomotor nerve). Her medical history was significant for hypertension and hypothyroidism. She was transferred to Providence St. Vincent Medical Center for further evaluation and treatment. Physical examinationOn admission, she had mild nuchal rigidity. Her mental status was normal. She had a complete right oculomotor nerve palsy with nonreactive pupil, ptosis and loss of all extraocular movements except for medial gaze. The remainder of her neurological exam was normal with regard to motor, sensory, cerebellar and reflex examination. Imaging findingsCerebral catheter angiography was performed urgently because of the known MRA finding of intracranial aneurysm. Angiography showed a large right posterior communicating artery aneurysm with significant mass effect on the third cranial nerve (Figure 1). Angiography also revealed a left ophthalmic artery aneurysm (Figure 3), a right pericallosal aneurysm and an anterior communicating artery aneurysm (Figure 1). The posterior communicating artery aneurysm was believed to be the only symptomatic lesion. The options of coil embolization and clip ligation were offered to the patient and family. Because of the mass effect of the aneurysm on the oculomotor nerve, surgical decompression of the nerve was favored. Surgical managementThe patient consented to undergo a right-sided craniotomy and clipping of the aneurysm with decompression of the oculomotor nerve. The patient was placed supine and under general anesthesia. A right frontotemporal craniotomy and modified orbitotomy was performed. The sylvian fissure was opened, and the arachnoid overlying the optic nerve and carotid artery was incised. After exposure of the internal carotid artery proximally and distally to the aneurysm, the neck of the aneurysm was identified and clip ligated. The aneurysm sac was decompressed to remove the mass effect on the oculomotor nerve. The anterior communicating artery aneurysm was also clip ligated. The patient had an uncomplicated postoperative course and was discharged home on postoperative day five. Post-operative angiography showed complete obliteration of the two treated aneurysms (Figure 2). At her two-month follow-up, her third-nerve palsy had completely resolved. The patient returned three months later and underwent uncomplicated coil embolization of the left ophthalmic artery aneurysm to complete obliteration (Figure 4). She was discharged home the following day without neurological deficits. Because of its very small size, the pericallosal artery aneurysm was left untreated and will be monitored with periodic MR angiograms. DiscussionMost cerebral aneurysms occur at points of bifurcation of major intracranial vessels, such as the anterior communicating artery, the posterior communicating artery and the middle cerebral artery. Multiplicity of intracranial aneurysms occurs in nearly a third of patients with cerebral aneurysms. Patients with multiple aneurysms carry a higher risk for future subarachnoid hemorrhage because the overall bleeding risk is cumulative. For this reason, greater consideration is given to treatment of aneurysms in these individuals. Acute onset oculomotor nerve palsy in a patient with a posterior communicating artery aneurysm is a harbinger of impending rupture if a subarachnoid hemorrhage has not already occurred. Abrupt expansion of the aneurysm through enlargement of the sac is one proposed mechanism. Also, partial localized hemorrhage and thrombosis adjacent to the nerve is an alternate pathway for development of ONP. These aneurysms must be secured urgently, if not emergently. Coiling embolization versus clip ligation of aneurysms causing an ONP is a point of great contention. Proponents of endovascular treatment point to the high rate of complete or partial return of third-nerve function as well as the safety of the less invasive endovascular approach. Surgical treatment may carry a higher rate of return of third-nerve function and may offer superior durability of aneurysm treatment when compared to endovascular therapy. Our philosophy with regard to these cases is patient-centric and individualized. Clipping is favored in patients in otherwise good health, younger patients and those with a complete third-nerve palsy. Coiling is favored for older patients in poor health with multiple medical co-morbidities. This patient underwent both treatments for separate aneurysms. She had an excellent outcome because these treatments were specific to her clinical characteristics and aneurysm morphology. Most importantly, treatment selection was independent of operator bias. |
|||||||||||||||||
|
|||||||||||||||||
|
Copyright © 2026 Providence Health & Services. All rights reserved. Clinical Trials | Quality and Outcomes | News and Events | About Us | Contact Us | Make a Referral |
|||||||||||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}