| Home News and Events |
|
eCardioVascular BeatWas the U.S. Surgeon General’s call to action on DVT justified?
W. Kent Williamson, M.D.
Chairman, Regional Endovascular Committee In September 2008, acting U.S. Surgeon General Steven Galson issued a This call to action was intended to raise DVT prevention to the highest national health care priority. Population-based studies indicate that up to 2 million people are diagnosed with DVT every year, with 200,000 to 300,000 of those dying from it every year. Perhaps one of the most startling findings was from a survey that revealed that up until a few years ago, only a third of hospitalized patients received appropriate prophylaxis for DVT. It is estimated that many thousands of lives can be saved once steps are taken to ensure prophylaxis. This information, combined with the high mortality rates, ultimately resulted in this call to action. The federal call to action was intended to stimulate a coordinated plan to reverse the current trend of noncompliance and to dramatically reduce morbidity and mortality. To accomplish this, multiple regulatory levels from hospital administration to federal agencies were engaged. The result? The Joint Commission and the Centers for Medicare & Medicaid Services now require providers to document compliance with prophylaxis measures. The end product in this endeavor has been to create specific medical-record documentation that compels the provider to outline the method of DVT prophylaxis for every hospitalized patient. If DVT prophylaxis is not opted for, clinical reasoning must be outlined. These forms usually combine an order set with areas for documentation in one page; this hopefully facilitates compliance. Projects such as the National Surgical Quality Improvement Program constantly analyze hospital and provider compliance while assessing the impact of greater compliance; with endpoints that include bleeding complication and incidence of DVT or pulmonary embolism. Is this fuss worth it? Given that deep vein thrombosis kills more people in the United States than HIV and breast cancer combined, and that DVT has flown under the radar for so long, many would say absolutely. Much of the initiative’s benefit is based on increasing awareness of risk factors, triggering events and preventive measures while empowering people to discuss their risk with their primary care provider. One method to increase community awareness has been to circulate a self-assessment tool, where individuals can familiarize themselves with risk factors for DVT and score that risk. The intention is that people will share risk information with providers and seek help early if any signs or symptoms of DVT arise. The U.S. Surgeon General’s task force estimates that tens of thousands of lives can be saved in the United States each year by making DVT and PE prevention our highest public health priority. 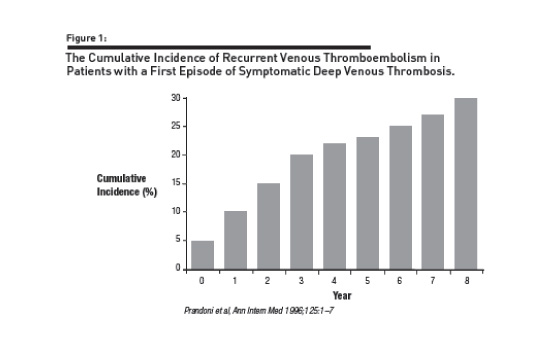 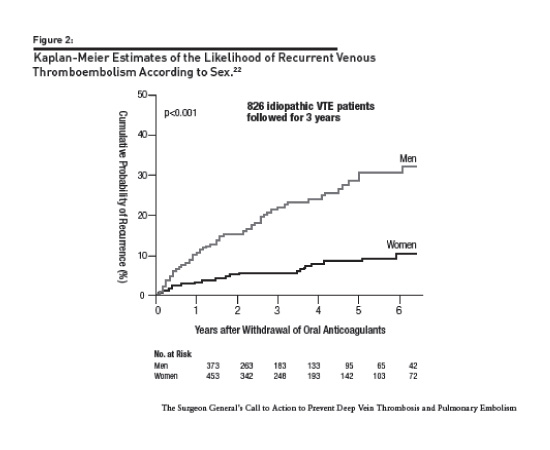 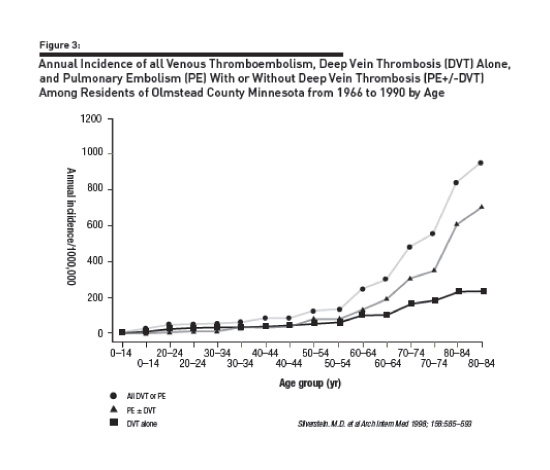 Charts reprinted from “The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism – 2008” Other articles by W. Kent Williamson, M.D. |
|||||||||||||||||
|
|||||||||||||||||
|
Copyright © 2026 Providence Health & Services. All rights reserved. Clinical Trials | Quality and Outcomes | News and Events | About Us | Contact Us | Make a Referral |
|||||||||||||||||